

Anyone who has discussed pedophilia or other minor attractions on social media has likely encountered the trope that individuals who are attracted to minors need to “get help”. The phrase has become a meme, littering the replies of any commentator who shares accurate information about minor attractions and the people who experience them. In most cases, it’s insincere; a thinly-veiled attempt to undermine rational discussion by implying that the target is so deeply disturbed that any further interaction would be pointless. It’s an ad hominem, attacking someone’s perceived mental state to avoid addressing their argument, and it’s therefore often overlooked as unproductive whining. However, beneath the snide remarks lies an important conversation, centered around a legitimate question: why don’t minor-attracted people (MAPs) just…“get help”?
Unsurprisingly, most people’s answer to this question is based on the widespread misconception that MAPs are generally in favor of child sexual abuse (CSA). Many believe that MAPs don’t seek support because they don’t want it or think they don’t need it. “After all,” the argument goes, “if someone was attracted to children but didn’t want to abuse them, wouldn’t they want to get help to avoid causing harm?” Despite its pervasiveness, this theory has long been disproven. A 2011 survey found that 58% of MAPs wanted to seek professional support but could not do so. Account for the MAPs who were able to get support and those who sought non-professional support, and it’s clear that a large majority of MAPs have some interest in getting “help.” So perhaps a better question is, what’s stopping them?
What is help for MAPs?
Depending on a MAP’s needs, help can take various forms. Some of the most common are therapy, self-help, support from friends and family members, and peer support from other MAPs. While the first three are generally considered acceptable forms of support, peer support for MAPs is controversial in public discourse, with some claiming that allowing MAPs to form communities will result in them becoming more likely to abuse children. This is despite experts repeatedly promoting the effectiveness of peer support as a tool for reducing some MAPs’ risk of offending and improving the wellbeing of others. Some child protection organizations have even gone so far as to partner with peer support groups for MAPs, further demonstrating their legitimacy as support resources. Unfortunately, studies showing that communities of child abusers can result in increased rates of abuse are often mistakenly applied to MAPs by individuals who lack expertise on the subject, usually due to a lack of knowledge that non-offending MAPs exist and make up a majority of MAPs. This warps public opinion on an important source of support and community for many MAPs.
It is important to note that not all MAPs require professional support. In most cases, peer support is sufficient to address any issues a MAP may encounter as a result of their attractions. The most recent editions of both the Diagnostic and Statistical Manual of Mental Disorders and the International Classification of Diseases reflect this fact by clarifying that pedophilic disorder (a treatable mental disorder, not to be confused with pedophilia) can only be diagnosed when a MAP is experiencing significant distress or engaging in harmful behavior due to their attractions. In both texts, pedophilia (an attraction to prepubescent children, not to be confused with pedophilic disorder) is depathologized, indicating that experts do not consider treatment necessary for MAPs who are not experiencing distress or engaging in harmful activities. Of course, seeking support is a personal choice, and some MAPs may want professional support even if they do not have pedophilic disorder.
Objectives of support
Much of the public’s confusion surrounding the distinction between pedophilia and pedophilic disorder is the result of misunderstanding the goals of professional support for MAPs. Contrary to popular belief, the goal of therapy for MAPs is not to change or eliminate their attractions. Conversion therapy is increasingly recognized as harmful and ineffective, with many identifying it as a form of torture, and minor attractions are no exception. One researcher even described the idea of curing MAPs as “dangerous,” explaining that it could give self-hating MAPs false hope, only to rip it away when such “treatments” fail, likely causing additional self-hatred and mental health issues.
According to experts, the main goal of professional support for most MAPs should be addressing the impacts of stigma. MAPs are constantly bombarded with hateful and misguided language, and this can lead to a variety of mental health issues. Anxiety and depression are common, and over 1 in 3 MAPs struggle with suicidal ideation. Minor MAPs are particularly susceptible, as demonstrated by the fact that the most common age for a MAP to first attempt suicide is just 14 years old.
In addition to negatively impacting MAPs, many mental health issues caused by stigma are known risk factors for sexual violence, meaning stigma may increase some MAPs’ risk of committing a sexual offense. Experts recommend that even prevention-focused MAP support initiatives center their messaging around improving mental health. This guidance is based on the finding that support initiatives that excessively focus on prevention may cause MAPs to view themselves as a danger and develop additional mental health issues that increase their risk of offending. Furthermore, MAPs who know they are not at risk of offending may view prevention-focused treatment programs as irrelevant to their needs, even when such programs could further improve their wellbeing.
Barriers to professional support
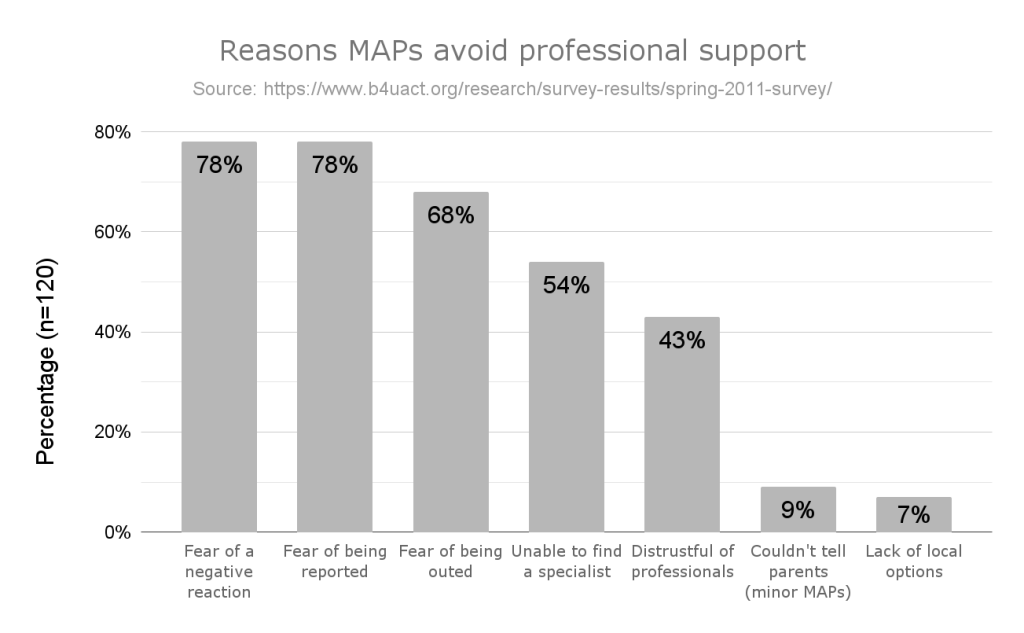
The 2011 survey mentioned above contained a question asking MAPs who wanted support but were unable to receive it what stopped them. The results are summarized in the graph above (respondents were allowed to select multiple answers, so the sum of percentages exceeds 100%) and were corroborated by a recent study on the support-seeking behaviors of MAPs. Notably, the more recent study also found that some MAPs who offended had attempted to seek therapy beforehand but encountered barriers that prevented them from receiving support. This backs up the growing consensus among experts that improving access to support for MAPs could lead to lower rates of child sexual abuse.
Harmful reactions
In both studies, the most common barriers MAPs encountered while seeking support were concerns about negative reactions from mental health professionals. Therapists are only human, and they are susceptible to the warped views and stigmatizing beliefs that often cause MAPs to need support in the first place. While some mental health professionals can set aside their biases and focus on their job, many fail to do so, potentially resulting in uncomfortable and dangerous situations for their clients. There have been reports of therapists insulting and belittling MAPs, falsely accusing them of offending, attempting to change their attractions, and, especially in the case of minor MAPs, violating patient confidentiality and informing their client’s family members about their attractions. All of these responses negatively impact MAPs’ mental health and may lead to the antisocial behavior that is often associated with sexual violence.
In extreme cases, therapists may report clients with minor attractions to law enforcement, even when there is no reason to suspect illegal activity. Mandatory reporting laws in most regions require therapists to report situations where there is an immediate or ongoing danger to a child. While there are serious issues with the effect these laws have on survivors, they should generally only directly impact people who have abused or plan to abuse a child. Unfortunately, most mental health professionals misinterpret their obligation and report MAPs by default, even though the vast majority of MAPs never offend. One study found that 24% of mental health professionals would report a MAP who had never offended and did not want to. These unnecessary reports can overwhelm the institutions designed to keep kids safe and can result in investigations that impact MAPs’ careers, relationships, and wellbeing, even when no evidence of illegal activity is discovered.
With such high stakes, many MAPs decide that professional support is not worth the risk
A harmful reaction from a mental health professional can lead to a MAP’s friends and family members learning about their attractions. Unlike mental health professionals, these people rarely have formal sensitivity training and are far more likely to believe misinformation and stereotypes that can cause them to mistreat the MAP they know. MAPs who are outed often lose jobs, housing, and relationships, and may even be cut off from their families, decimating their already-limited support systems. With such high stakes, many MAPs decide that professional support is not worth the risk.
Inability to find support
Even when MAPs are willing to take on the risks associated with seeking support or reduce those risks by looking for therapists who specialize in minor attractions, they have limited options. There are organizations dedicated to helping MAPs find safe therapists, such as those listed on the Prostasia Foundation’s Get Help page, but most MAPs and mental health professionals are unaware of their existence. When MAPs do discover them, their lists are short, often containing no more than a couple of therapists for each region. Making matters worse, mental health professionals are increasingly facing backlash for supporting evidence-based child sexual abuse prevention efforts, reducing the number of therapists who are comfortable being listed by these organizations.
In addition to reducing a MAP’s chances of finding a compatible therapist, the lack of options can exacerbate more widespread issues with mental healthcare. MAPs may not be able to find a therapist who accepts their insurance or charges a reasonable rate when choosing from the few safe providers in their area. According to a 2018 study, 23% of MAPs who wanted professional support but could not receive it encountered financial difficulties. Because lists of safe therapists are often only separated into large regions, MAPs may be unable to travel the distance required to see a therapist who is technically in their region. Furthermore, when there are only a few safe therapists available for highly-populated areas, they may be overwhelmed by the number of MAPs seeking support, leaving some MAPs without treatment.
Minor MAPs who want professional support face the additional obstacle of needing parental permission (and funding) to see a therapist. As previously mentioned, disclosing attractions to family members can be dangerous for MAPs. Some parents may react in abusive or otherwise harmful ways rather than helping their children get the support they need. While this problem is not unique to MAPs, minor-attracted people do not have the backing of institutions that have been established to support members of many other marginalized groups in similar situations.
Other barriers to support
MAPs seeking non-professional forms of support also face obstacles. Chief among these is censorship. In recent years, mainstream social media platforms have repeatedly banned MAP-focused support groups, child protection experts, and mental health professionals without explanation, even when the accounts in question have never violated their rules. Hoping to deter such actions, experts have publicly informed the companies about the potential harm, but platforms have ignored these efforts, opting to prioritize their public image over child safety.
CSA prevention experts face a similar issue in the form of backlash to their evidence-based approach. Many will remember Allyn Walker, the award-winning researcher who was forced out of their position at Old Dominion University after their interview on the benefits of destigmatizing MAPs and previous work in prevention were grossly misrepresented by critics and the media. These overreactions to uncomfortable facts about abuse even harm CSA survivors, such as the member of the Scottish Parliament who received death threats after correctly explaining that abusers are often friends and family members of their victims. Events like these discourage people, including survivors, from spreading accurate information, which impedes all prevention efforts.
Overcoming the hypocrisy of “Get help!”
As previously established, the phrase “get help” is typically insincere when directed at MAPs or experts on minor attractions. It is often used by the same people who perpetuate the stigma that causes many MAPs to need support and prevents most from receiving it. If the people telling MAPs to “get help” truly wanted MAPs to receive support, they would recognize the long-standing evidence that the problem isn’t a lack of MAPs who want support, but rather the stigma-based barriers that prevent them from pursuing that support. Instead of repeating a catchphrase, they would spread accurate information about minor attractions and the support available to MAPs, making it safer and easier for MAPs who want help to find it.
Increasing the ability of minor-attracted people to access support would have widespread benefits. In addition to improving the wellbeing of MAPs, it would reduce the prevalence of mental health issues that can lead to sexual violence and likely reduce rates of child sexual abuse overall. More MAPs engaging with the mental health community would allow researchers who study MAPs to have larger and more representative samples, leading to more reliable findings about the role of MAPs in CSA prevention efforts. Support groups for MAPs would become more effective as their membership grew and became more diverse. If the increased access was a result of decreased stigma, accurate information about prevention would become more widespread than ever, and the number of MAPs in need of support would decrease, reducing strain on mental healthcare providers.
Every child is safer when people take the time to learn the basics of preventing abuse
A world with improved access to support for MAPs, widespread knowledge on CSA prevention, and reduced rates of abuse may seem like a distant dream, but there are simple steps most people can take today to help make it a reality. First and foremost, do your research. Every child is safer when people take the time to learn the basics of preventing abuse. Avoid using language that perpetuates stigma or reinforces false assumptions, and develop methods to identify misinformation. If you know someone who is a MAP, set aside time to learn how you can support them while also addressing your own mental health needs. Finally, and most importantly, talk about your experiences to whatever extent you feel comfortable.
Whether you’re a CSA survivor, minor-attracted person, mental health professional, child protection expert, or any combination of those, your voice matters in this fight. Both child abuse and mental health issues thrive when discussions about them are silenced by stigma, shame, and fear. It is only by speaking up and providing a space for others to do the same that we can bring about a better, safer world.
Correction: A previous version of this article wrongly stated that 75% of mental health professionals wrongly believed that mandatory reporting laws required them to report all MAPs. This has been replaced with more accurate wording above.
If you or someone you know struggles with attractions to minors, you can find support and resources here.
Basically this:
The response could then be:
Alternatively:
That last one is from: https://www.pacialife.com/post/the-mental-health-stigma-from-a-college-student-perspective
I’m not saying that this accurately describes my situation, but I don’t need prevention-focused treatment because such programs are irrelevant to my needs. Although, some support would be nice.
Replace the word “epilepsy” or “seizure” with “minor-attracted person” or “pedophilia” in these memes:
They probably don’t make much sense, especially that last one, but I thought they were still kinda relevant. Given how many “anti-MAP” memes there are, I had to use something else.
… stigma, shame, and fear.
I mean the fight against abuse and CSAM has derailed completely. It’s pretty much become a tool to limit basic rights and push an agenda. There are no increase in police enforcement rather it’s symbolic laws. Where did prevention go?
How can you publicly defend anything that is even slightly associated with it, without risking your life. Politicians who actually stick to their core values such as liberty and “no moral influence in criminal law” are getting rarer, because now with the internet any morally wrong stance is going to ruin you. It’s not about what might be good, but what sounds good. All this collateral damage alone; people who thought they’d never come into contact with laws “against” MAPs. Take the one guy from the UK who ordered a busty doll, but it was below 160cm making it illegal. Same is gonna happen with Anime on a broader scale.
This might be a good time to suggest that we change the “Get Help” link & thumbnail on Prostasia’s homepage to something like “Want Help” instead?
Tbh I kinda like the fact that it rebrands the phrase to actually providing support resources. It makes it an option, rather than a command
I can see the thought process behind that, however my problem with it is that most people probably won’t click to see the options on the page so they’ll assume its a command anyway no?
Like its only a rebrand if people actually click and read it to see what it says otherwise they’ll assume the derogatory meaning which might be a little demotivating to Map’s who are new to the site and don’t need help if that makes sense? Just my opinion anyway lol